
Significance
Necrotic myocardium does not fail in a single way after coronary occlusion. Cardiomyocyte death initiates inflammation, matrix remodelling, vascular responses, and fibroblast activation all at once, however, bulk tissue measurements flatten those events into averages and obscure the cells that may decide whether the ventricle scars, stabilizes, or partially recovers. The scientific question is not simply which cells appear after myocardial infarction, but which chromatin programs become accessible as repair unfolds, and how those programs relate to cell fate. Fibroblasts have long been thought of as central executors of scar formation, but their behaviour during repair remains not fully understood. They are heterogeneous, temporally plastic, and exposed to a damaged environment that can push them toward matrix deposition, mechanical support, or lineage-adjacent states that are harder to classify. Transcript data alone can register gene expression, but it cannot fully reveal the regulatory architecture that permits one fibroblast population to remain fibrotic while another moves toward a more developmentally charged identity. In a recent research paper published in Cardiovascular Research, Dr. Shuchen Zhang, Dr. Boyang Xiang, Dr. Yiheng Zhao, and led by Professor Xiang Zhou from the Second Affiliated Hospital of Nanjing Medical University working together with Dr. Wenjing Wang and Dr. Lili Chen from the Second Affiliated Hospital of Soochow University, examined cardiac repair after myocardial infarction using integrated single-cell epigenomic and transcriptomic analysis. Their work resolved regulatory fibroblast states that are not easily captured by transcript profiling alone. They identified a GATA5/ISL1+ fibroblast population with mixed fibroblast and cardiomyocyte features, distinct from transient Gli3 high fibroblasts and from conventional myofibroblasts. They also built a fibroblast-targeted adenoviral overexpression strategy and connected its repair-associated effects to repression of the Rspo1–β-catenin–TCF4 arm of Wnt signalling in mouse and human cardiac fibroblasts.
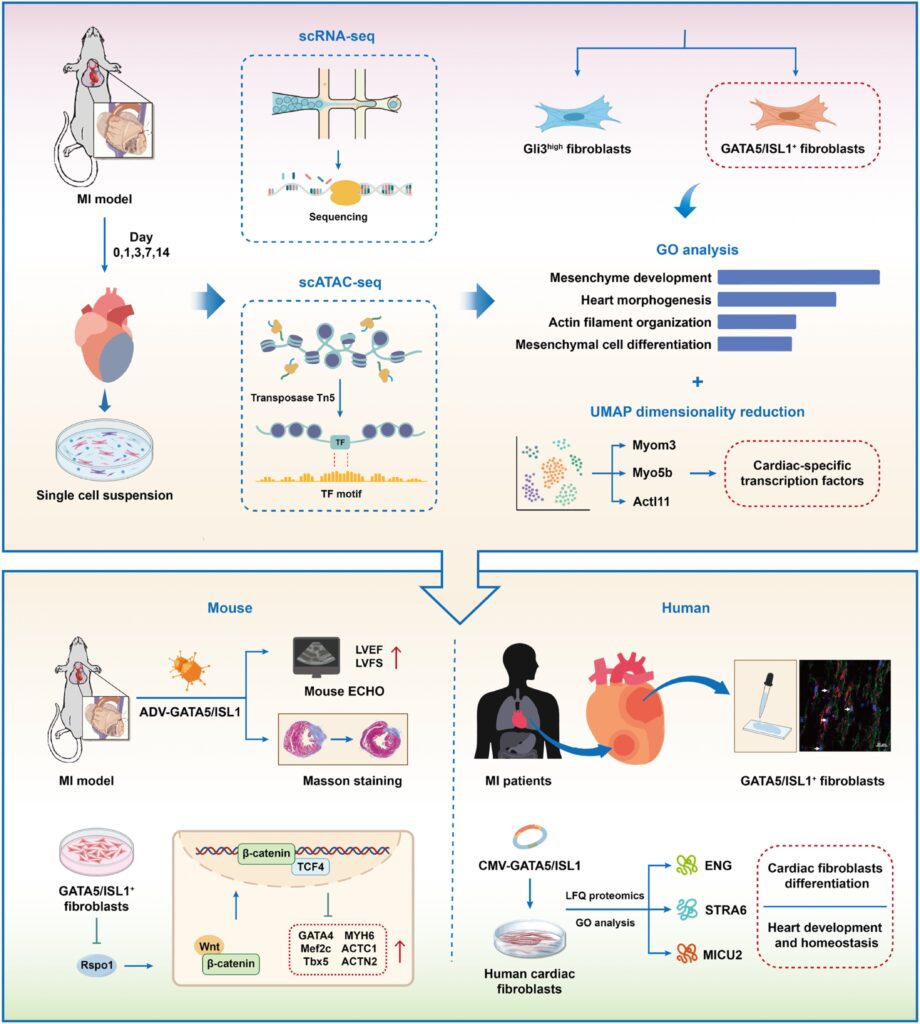
This is why the authors combined scATAC-seq with scRNA-seq in mouse hearts collected across the early and intermediate phases after left anterior descending coronary ligation, and why they extended the logic of the study into human post-infarct tissue. The design carries a clear intellectual motive. Myocardial repair is not static, and any attempt to understand it without temporal resolution risks confusing transient intermediates with stable cell types. The same issue applies to fibroblasts: a population identified late after infarction may have emerged through several short-lived states that leave regulatory traces even when the transcriptional signal has already shifted. By linking chromatin accessibility to gene activity and transferred RNA labels, the investigators placed cell identity and regulatory potential into the same analytical frame. If fibroblast behaviour is controlled by a sequence of regulatory openings and closures, then the path into repair becomes as important as the final scar itself.
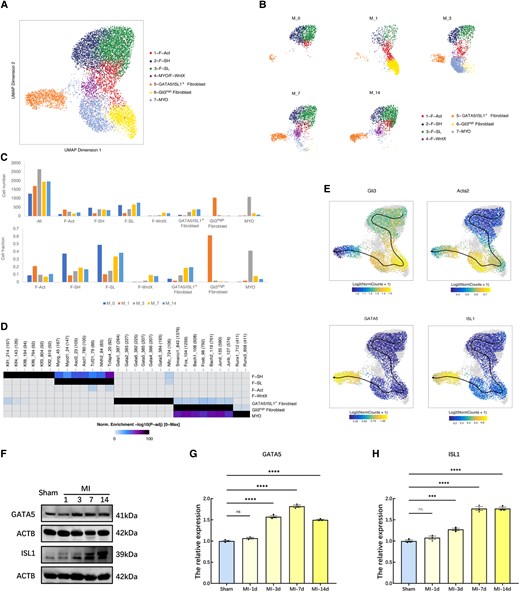
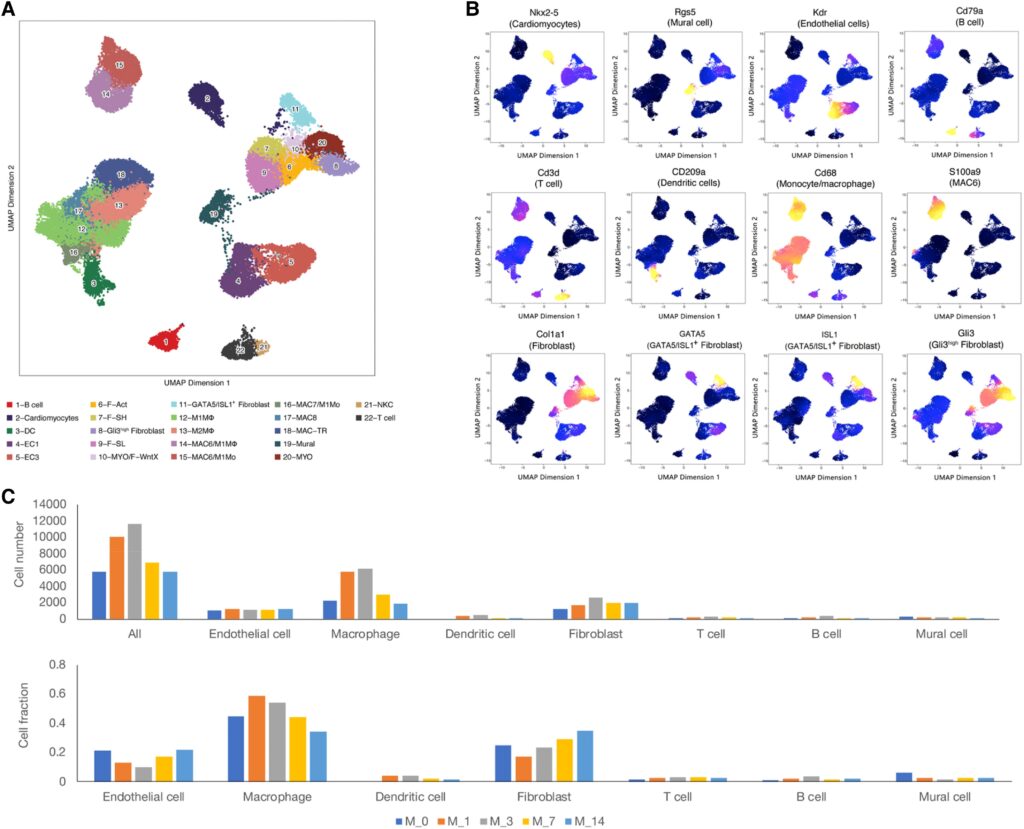
The research team generated scATAC-seq profiles from control hearts and from infarcted hearts sampled at 1, 3, 7, and 14 days, then integrated those data with reference scRNA-seq to annotate cell states across more than 40,000 cells. They identified the expected endothelial, mural, immune, lymphoid, and fibroblast populations, yet the analysis also separated two fibroblast groups that had not been resolved in the prior transcript-only framework: a Gli3high population and a GATA5/ISL1+ population. The investigators observed immediate monocyte/macrophage expansion after infarction, peaking early and subsiding by day 14, while fibroblasts followed a different rhythm, shrinking at day 1 under the weight of inflammatory influx and then expanding through later repair.
The authors then focused on fibroblast lineage structure. They found that activated fibroblasts rose as Sca1-high and Sca1-low fibroblasts declined, while myofibroblasts surged early and then receded. Gli3high fibroblasts appeared briefly and carried a chromatin program close to myofibroblasts, which led the investigators to treat them as a transitional state. GATA5/ISL1+ fibroblasts behaved differently. Their abundance increased from day 3, plateaued by day 7, and still accounted for about one-fifth of fibroblasts at day 14, outlasting both myofibroblasts and Gli3high cells. The researchers linked this population to mesenchymal development, heart morphogenesis, actin filament organization, and mesenchymal differentiation, and they found chromatin and motif similarity to both myofibroblasts and cardiomyocytes. That mixed signature is scientifically interesting because it does not fit the usual binary choice of fibrotic versus muscle. It reads more like a repair state under developmental pressure, still tethered to fibroblast identity but no longer confined by it.
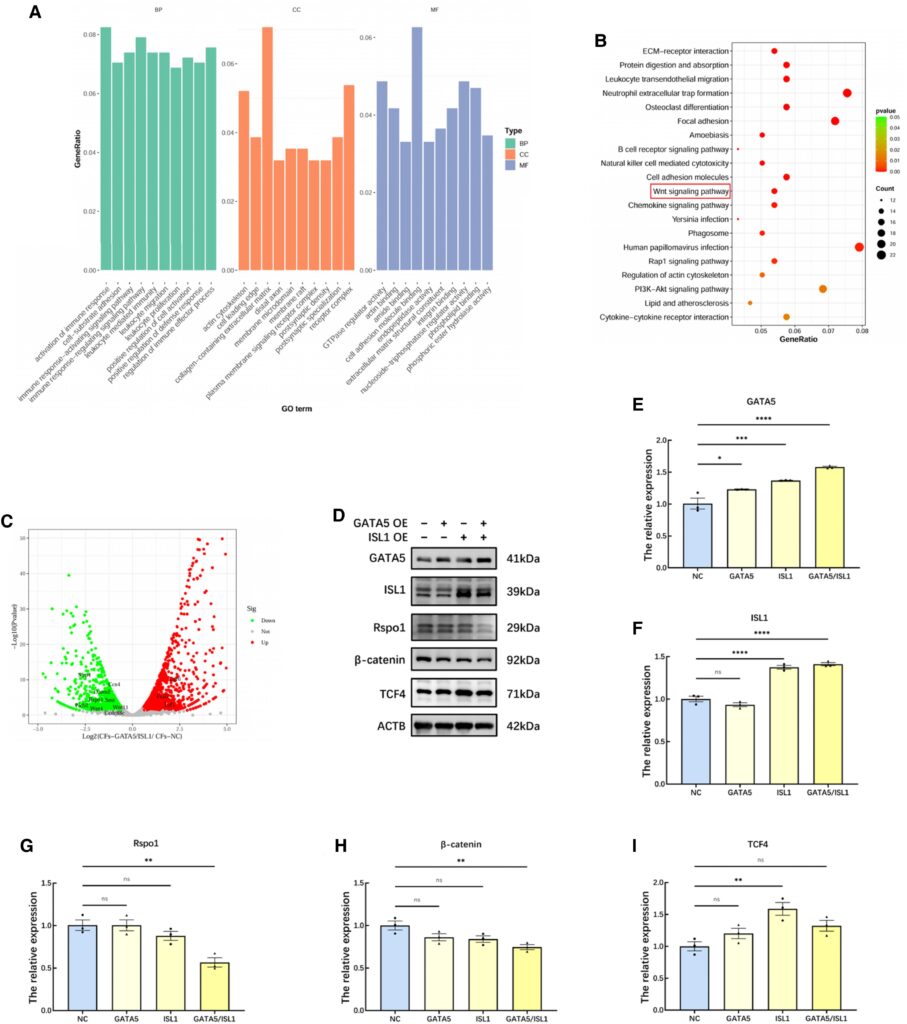
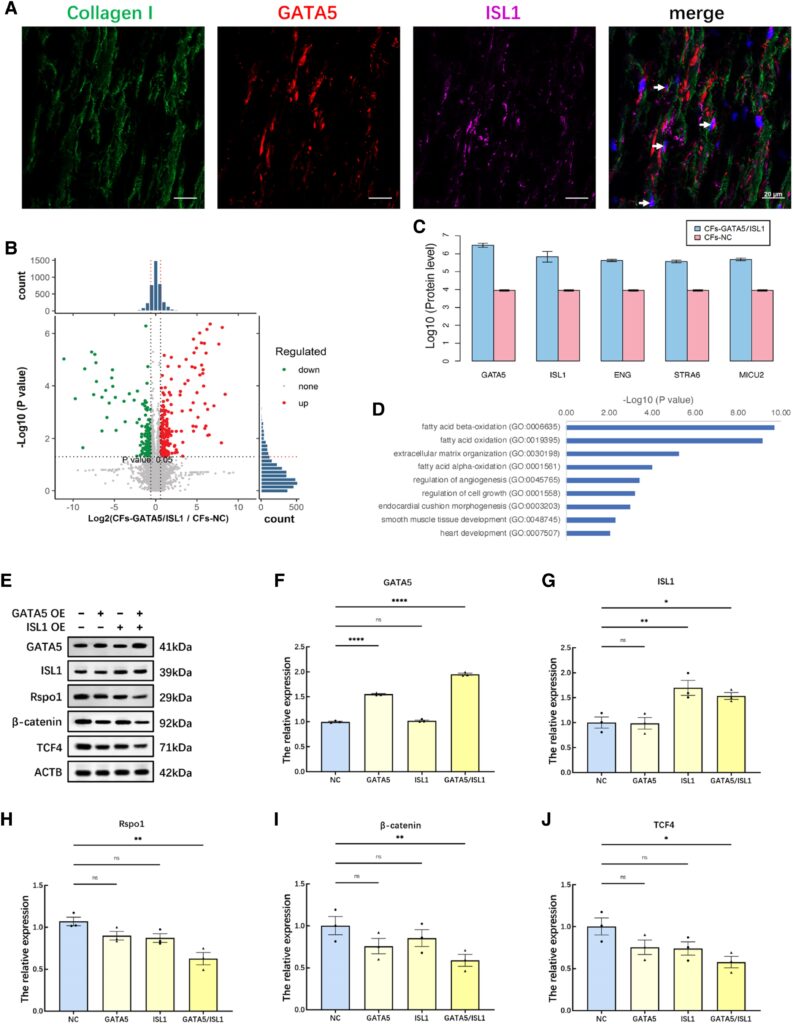
The study examined mechanism and function in parallel. They connected GATA5 occupancy with downstream target gene scores, and immunostaining confirmed the appearance of GATA5/ISL1+ fibroblasts in infarcted tissue. The investigators also detected cardiac transcription factors and muscle-associated genes in these cells, which strengthened the argument that they had acquired part of a cardiomyocyte-like program. To test whether this state could influence repair, the authors drove GATA5 and ISL1 expression in cardiac fibroblasts using an adenoviral system built around a collagen promoter. They observed improved ventricular function trends, less fibrosis, smaller infarcts, and enrichment of GATA5/ISL1+ fibroblasts in the infarct border zone. Forced expression helps clarify the biological axis, while the endogenous programme likely follows a more context-dependent course. Even so, the concordance between the endogenous single-cell data and the intervention data gives the argument unusual weight. RNA-seq and protein analysis then pulled the mechanism toward Wnt control, with reduced Rspo1, β-catenin, and TCF4 accompanying GATA5/ISL1 expression. Human scar tissue contained GATA5/ISL1+ fibroblasts as well, and proteomics in human cardiac fibroblasts linked the same axis to cardiac development, homeostasis, angiogenesis, matrix regulation, and fatty acid oxidation.
What makes this paper matter is that it shifts the conversation about post-infarct fibroblasts away from a single-path scar narrative. Fibroblasts in the injured heart are often discussed as drivers of collagen deposition, mechanical stabilization, and later stiffness, all of which are true. Professor Xiang Zhou and colleagues demonstrated that at least one fibroblast state carries a regulatory program closer to tissue reconstitution than to terminal fibrosis. That does not mean the infarcted heart is naturally regenerating in any broad sense. It means the repair field may contain a narrower, temporally restricted cell population whose chromatin state permits partial movement toward a cardiomyocyte-like transcriptional identity. It opens the door to design principles based on timing, transcription factor combinations, and cell-state conversion, instead of the familiar attempt to suppress fibroblast activity wholesale.
By merging chromatin accessibility with transcript data, the authors show that repair biology after myocardial infarction cannot be fully understood from expression matrices alone. Regulatory potential leaves a signal before terminal phenotype becomes obvious, and transient intermediates may be visible in one modality more clearly than the other. The identification of Gli3high fibroblasts as a short-lived state and GATA5/ISL1+ fibroblasts as a later, more persistent state illustrates that point well. For cardiac biology, this matters because repair is a staged process; a cell that appears only briefly may still determine what comes next. For therapeutic thinking, the novel work implies that interventions aimed at fibroblasts may need to discriminate among fibroblast states with much finer temporal resolution than current anti-fibrotic strategies usually allow. A program that is beneficial in the border zone during one repair window could easily be lost, or misread as noise, in coarser analyses. The translational implications are promising and the appearance of the same fibroblast state in human scar tissue gives the study a confirmation beyond rodent inference. The Wnt-associated regulatory axis is equally important. If GATA5/ISL1-dependent suppression of the Rspo1–β-catenin–TCF4 arm of Wnt signalling marks a route by which fibroblasts loosen their fibrotic program and acquire cardiac features, then future work could treat that axis as a target for selective reprogramming, provided cell targeting and timing can be handled with precision.
![]()
![]()

Reference
Zhang S, Xiang B, Zhao Y, Wang W, Chen L, Zhou X. Single-cell epigenomic and transcriptomic analysis unveils the pivotal role of GATA5/ISL1+ fibroblasts in cardiac repair post-myocardial infarction. Cardiovasc Res. 2025;121(9):1419-1432. doi: 10.1093/cvr/cvaf101.
Go to Journal of Cardiovascular Research