
Significance
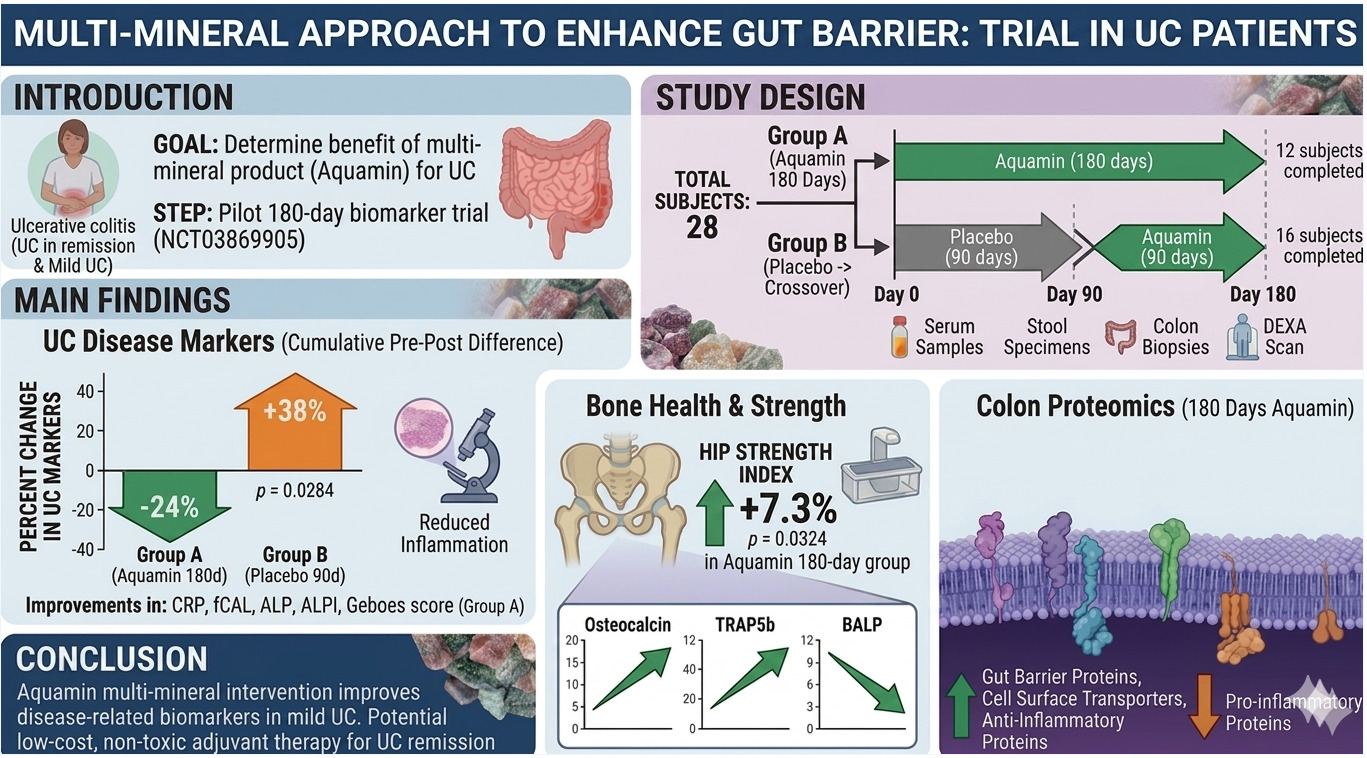
Ulcerative colitis is a chronic inflammatory bowel disease marked by ulceration, bleeding, abdominal pain, diarrhea, and recurrent periods of flare and remission. Treatment with biologics and targeted small molecules has improved clinical care, but substantial residual pathology often persists in patients with mild-to-moderate disease. Earlier animal experiments have linked a multi-mineral product derived from calcified red marine algae to reduced gastrointestinal inflammation and fewer neoplastic lesions, while organoid studies using human colon tissue had shown increased expression of proteins involved in gut barrier structure and reduced expression of proteins associated with pro-inflammatory signaling. A prior biomarker study in healthy adults moved this question one step closer to the clinic, demonstrating that some of these same tissue-level protein shifts could also be detected in human colonic biopsies after oral intake. Importantly, ulcerative colitis also carries consequences beyond the colon. If chronic bowel disease changes inflammation, absorption, and mucosal physiology over prolonged periods, then a mineral-based intervention might affect more than one disease-related axis simultaneously. In a recent research paper published in PLoS One, Muhammad Aslam and colleagues (Danielle Kim Turgeon, Henry Appelman, Ryan Stidham, Shannon McClintock, Ron Allen, Gillian Moraga, Isabelle Harber, Kara Jencks, Molly McNeely, Ananda Sen, Karl Jepsen, and James Varani) at the University of Michigan Medical School designed a randomized 180-day biomarker trial, pairing a marine red algae-derived multi-mineral intervention with serial blood, stool, colon biopsy, mucosal proteomics, and Dual-energy X-ray absorptiometry (DEXA) measurements in ulcerative colitis patients before and after the intervention.
Briefly, the investigators ran a single-site, double-blind, randomized, placebo-controlled crossover trial in 28 participants with UC in remission or with mild disease. They assigned 12 participants to Aquamin for the full 180 days and 16 participants to placebo for 90 days, followed by crossover to Aquamin for the final 90 days, while all participants continued their usual maintenance therapy. The team collected blood, stool, and sigmoid biopsies at baseline, day 90, and day 180, and included DEXA imaging at baseline and day 180 to capture skeletal effects that shorter intervals would likely miss. Their design recognized that barrier biology, inflammatory activity, and bone remodeling do not move on the same timescale. The research team measured serum chemistry markers, C-reactive protein, intestine-specific alkaline phosphatase, fecal calprotectin, histologic injury, bone turnover markers, and mucosal proteomic profiles. They found little change across the standard safety chemistry panel apart from alkaline phosphatase, which fell by 9% after 180 days of Aquamin and rose slightly in the placebo group. They then separated the intestine-specific isoform and found the same directional split: ALPI decreased by 10% with Aquamin over 180 days and increased by 17% with placebo. The investigators also tracked inflammatory burden through CRP and fecal calprotectin. CRP declined by 24% in the 180-day Aquamin arm while the placebo group showed a small increase, and fecal calprotectin dropped by 29.4% with prolonged Aquamin exposure while rising by 43% under placebo. The pathologist recorded low baseline scores in most biopsies, which fits the mild-disease population, but Aquamin still shifted the simplified Geboes score downward by 48%, whereas placebo pushed it upward by 121%. When the authors combined these five biomarker changes into a composite measure, they achieved statistical significance between the groups.
In parallel, the researchers profiled mucosal biopsies using mass spectrometry-based proteomics and focused on proteins linked to epithelial differentiation, barrier assembly, inflammation, and electrolyte transport. They found increased expression of keratins and filamin; mucus-layer proteins such as MUC2, FCGBP and ZG16; tight-junction-associated proteins including TJP1 and JAM-A; multiple cadherins (including CDH1 and CDH17); and desmosomal proteins (DSC2, DSG2, and DSP). They also identified higher expression of EPCAM, CHL1, and basement-membrane components, consistent with tissue shifting toward stronger epithelial organization. At the same time, the investigators observed reduced levels of proteins tied to inflammatory drive or neutrophil activity, including PLA2G2A, JAK1, lactotransferrin, and NCF1, while proteins associated with counter-inflammatory control or mucosal homeostasis, including SMAD4, PIGR, MEP1A, tissue ALPI, and several carbonic anhydrase isoenzymes, moved upward. They also noted upregulation of transport-related proteins, including Na⁺/K⁺-ATPase subunits (ATP1B1 and ATP1B3); CLCA1/4 and CLIC5, and multiple SLC family members including SLC26A3 (also known as DRA).
Lastly, the study team also examined bone outcomes in parallel with the intestinal biomarkers. The authors measured femoral neck and lumbar spine parameters by DEXA and paired those readouts with serum bone turnover markers such as osteocalcin, TRAP5b, and bone-specific alkaline phosphatase (BALP). After 180 days of Aquamin intake, they observed a 1% increase in femoral neck bone mineral density (BMD) and a 3% increase in bone mineral content (BMC), contributing to a 7% gain in the calculated hip strength index. This is notable because, with many pharmaceutical interventions, achieving comparable improvements in BMD and BMC often takes a couple of years. The investigators then found a matching bone remodeling pattern in serum: osteocalcin rose by 34%, TRAP5b rose by 22%, and BALP fell by 9%, while placebo moved in the opposite direction or showed little change. Bone turnover is rarely captured through one perfectly synchronized marker, and the authors addressed that complexity by comparing the composite behavior of the marker set instead of over-interpreting any one analyte.
To summarize, the study by Muhammad Aslam and colleagues showed improvement in several biomarkers under the mineral intervention, and the proteomic results, the shifts in fecal calprotectin and histology, and the movement in intestine-linked alkaline phosphatase converge on a more layered interpretation: mucosal stability may change when epithelial architecture, mucus production, tight-junction support, and ion transport move in a coordinated direction. Drug development for ulcerative colitis usually focuses on stronger immune suppression or more selective cytokine control. However, the intervention seems to work by altering the mucosal setting in which inflammation persists, and this reflects a different therapeutic logic. If future trials confirm these observations, one could imagine mineral-based support entering maintenance strategies not as a replacement for established treatment, but as a means of shifting the tissue environment away from chronic fragility. In a cohort without dramatic baseline inflammation, the biomarker shifts still support a meaningful biological signal. The authors’ bone findings extend the relevance of the study beyond intestinal inflammation alone. Ulcerative colitis-associated bone loss is usually treated as a complication to monitor, not as a process linked back to the same intervention being tested for intestinal health. Aquamin shifted femoral neck mineral accrual, hip strength index, and bone turnover markers in a direction consistent with active remodeling and improved structural status over six months. Still, the findings raise a practical possibility: a well-tolerated adjunct that affects both mucosal biomarkers and skeletal endpoints could be especially relevant for patients whose disease remains clinically quiescent while extraintestinal burdens accumulate slowly over years. Barrier repair is one important theme in ulcerative colitis, and fluid absorption and electrolyte handling also shape bowel function in direct ways. When the authors report increased expression of SLC26A3 and ATPase subunits involved in ion gradients, they open a second mechanistic path for symptom benefit which may be considered less dramatic or complex than cytokine biology, though perhaps closer to how patients feel from day to day. If later trials connect these transporter changes to stool pattern or urgency, the medical field may need to rethink mucosal physiology as an attractive treatment target, not just inflammation biomarkers.
Reference
Aslam MN, Turgeon DK, Appelman HD, Stidham R, McClintock S, Allen R, Moraga G, Harber I, Jencks KJ, McNeely MM, Sen A, Jepsen KJ, Varani J. A multi-mineral intervention to improve disease-related and mechanistic biomarkers in ulcerative colitis patients: Results from a randomized trial. PLoS One. 2025;20(12):e0337408. doi: 10.1371/journal.pone.0337408.
Go to PLoS One.