
Dopamine replacement therapy remains the cornerstone of symptomatic management in Parkinson’s disease, offering substantial relief of motor impairment for many patients. Yet, even among individuals with clinically and pathologically confirmed disease, responses to dopaminergic medication vary widely. Some patients experience dramatic improvements in movement, while others show only modest benefit or develop complex side effects that limit therapeutic gain. This heterogeneity has long posed a challenge to clinicians and has complicated efforts to refine treatment strategies beyond empirical dose adjustments. Historically, variability in dopamine responsiveness has been attributed primarily to differences in disease stage, dopaminergic neuronal loss, or pharmacokinetics. While these factors undoubtedly contribute, they do not fully explain why patients with comparable clinical profiles and medication exposure can diverge so markedly in outcome. Increasingly, attention has turned toward broader network-level effects of dopamine replacement, particularly its influence beyond the classical nigrostriatal motor circuit. Dopaminergic medications do not act selectively on the basal ganglia; rather, they engage multiple dopaminergic pathways, including mesocortical and mesolimbic systems that project widely across the cerebral cortex. Cortical neurophysiology is tightly coupled to dopaminergic tone, especially through oscillatory dynamics that govern motor control, cognition, and behavioral flexibility. Among these rhythms, beta-frequency activity occupies a central role in Parkinson’s disease pathophysiology. Excessive beta synchronization is associated with motor rigidity and bradykinesia, whereas its normalization is commonly linked to clinical improvement following dopaminergic treatment. However, beta activity is not confined to sensorimotor cortex, nor is its modulation uniformly beneficial across cortical territories. This raises a critical but underexplored question: could dopaminergic enhancement of beta activity in non-motor cortical regions contribute to diminished therapeutic response? Addressing this question has been technically challenging. Traditional neuroimaging approaches often average responses across individuals, obscuring meaningful interindividual differences. Moreover, separating intended dopaminergic effects on motor circuitry from unintended engagement of cortical dopamine systems requires both high temporal resolution and a principled framework for linking physiology to neurochemical architecture. Without such tools, cortical contributions to treatment variability have remained largely speculative. To this account, new research paper published in Movement Disorders and led by Professor Alex Wiesman from the Simon Fraser University in collaboration with Dr. Mikkel Vinding, Panagiota Tsitsi, Per Svenningsson, Josefine Waldthaler, and Professor Daniel Lundqvist from the Karolinska Institutet, the researchers developed a neurophysiological framework that links individual cortical responses to dopamine replacement therapy with underlying cortical dopamine system architecture. By integrating pharmaco-MEG, spectral parameterization, and neurochemical atlases, they revealed that beta-frequency enhancement in dopamine-rich cortical regions predicts poorer clinical response. This work identifies unintended cortical dopaminergic overactivation as a previously unrecognized contributor to treatment variability in Parkinson’s disease. More broadly, it establishes a scalable strategy for contextualizing medication effects within distributed neurochemical networks.
The research team analyzed resting-state magnetoencephalography recordings acquired from patients with mild-to-moderate Parkinson’s disease both before and after administration of their usual dopaminergic medication. Healthy older adults underwent parallel recordings to control for nonspecific session effects. Clinical motor function was quantified immediately following each scan using standardized motor rating scales, allowing direct linkage between neurophysiological changes and symptomatic response.
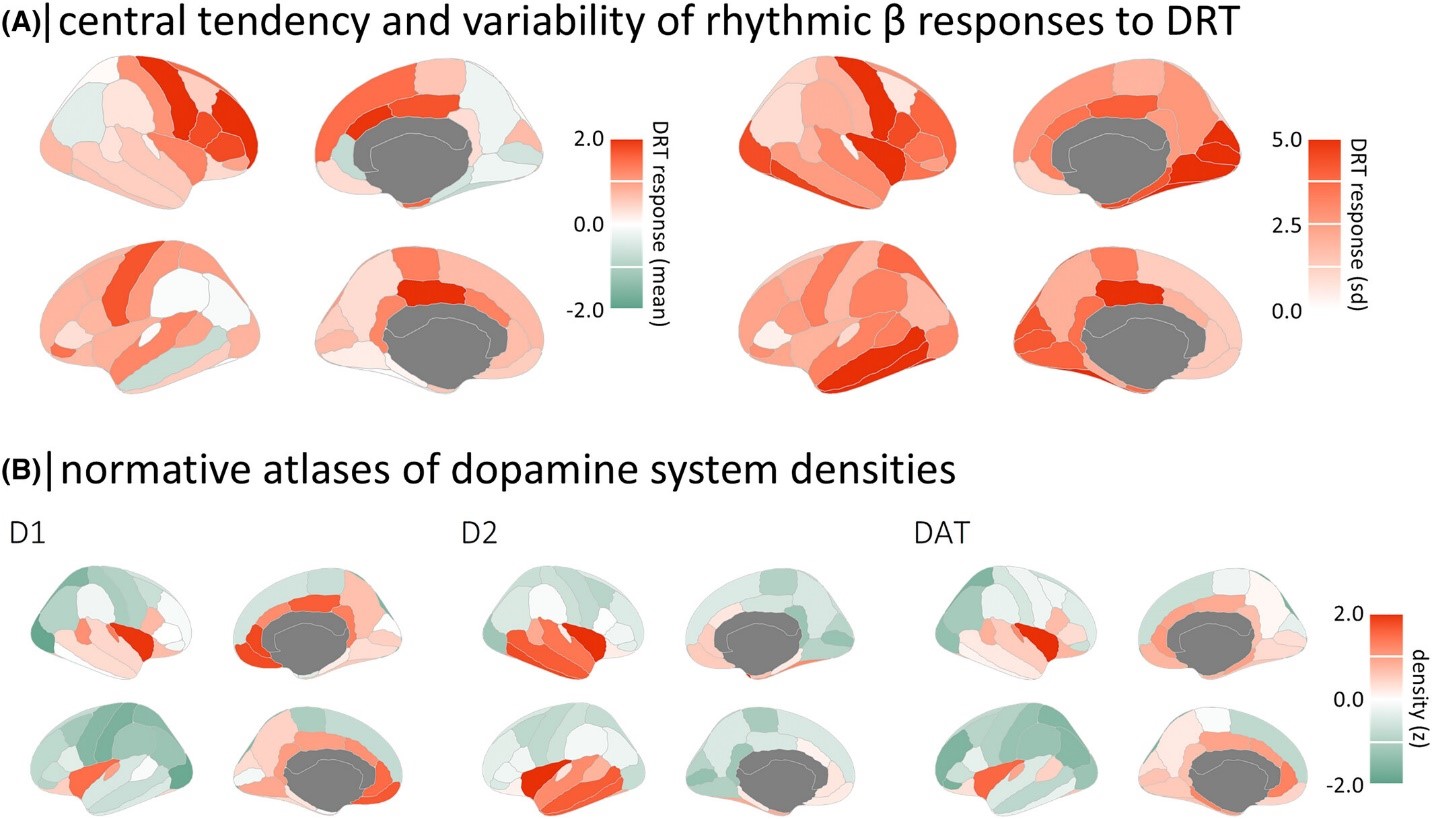
The authors reconstructed cortical activity at the source level and parcellated into anatomically defined regions. Rather than relying on raw spectral power alone, the authors applied spectral parameterization to disentangle rhythmic oscillations from the aperiodic background signal. This distinction proved crucial, as it allowed selective examination of dopamine-sensitive rhythmic components without conflation by broadband changes in neural noise. The analysis focused primarily on beta-frequency activity, while also evaluating alpha and arrhythmic features to assess specificity. They generated individual maps of dopaminergic response by contrasting post-medication and pre-medication cortical activity and then normalizing these differences relative to healthy controls. These maps revealed substantial interindividual variability, particularly in beta-band responses, with some patients showing pronounced cortical enhancement and others exhibiting minimal change. Notably, the spatial distribution of this variability was not random. Regions displaying the greatest intersubject differences overlapped strikingly with cortical areas known to express high densities of dopamine receptors and transporters. Afterward, the authors employed a partial least squares framework that related spatial patterns of neurophysiological change to normative dopamine system atlases. This multivariate approach identified a robust alignment between beta-frequency enhancement and dopamine-rich cortical regions, an effect that was absent for alpha rhythms, slower frequencies, and aperiodic activity. The alignment indicated that, in a subset of patients, dopamine replacement selectively amplified beta oscillations in associative and frontal cortical areas heavily innervated by mesocortical dopamine pathways. Crucially, the strength of this cortical dopaminergic engagement carried clinical consequences. Patients who exhibited greater beta enhancement in dopamine-dense cortical regions experienced smaller improvements in motor symptoms following medication. This inverse relationship persisted after accounting for symptom laterality and medication dose, and it was specific to treatment-related changes rather than baseline severity. Furthermore, the effect was most closely associated with axial and non-lateralized motor features, consistent with a mechanism distinct from classical contralateral motor cortex modulation.
In conclusion, the new study offers a conceptual shift in how variability in dopaminergic treatment response is understood in Parkinson’s disease. Rather than framing non-responsiveness as a failure of dopaminergic restoration per se, the findings suggest that excessive or misdirected cortical dopaminergic engagement may actively counteract therapeutic gains. In this view, dopamine replacement is not uniformly beneficial or detrimental, but context-dependent, shaped by the spatial pattern of its cortical effects. Moreover, the identification of beta-frequency enhancement in dopamine-rich cortical regions as a negative predictor of clinical response has important mechanistic implications. Beta oscillations have long been implicated in Parkinsonian motor impairment, yet their role has typically been interpreted within the confines of sensorimotor circuitry. By demonstrating that similar rhythmic dynamics in non-motor cortical areas relate inversely to treatment efficacy, the present work highlights the functional heterogeneity of beta activity across the cortex. Beta is not inherently pathological or therapeutic; its impact depends on where it emerges and which circuits it entrains.
From a clinical standpoint, these results point toward the possibility of stratifying patients based on their cortical neurophysiological response profiles. Non-invasive measures such as magnetoencephalography could, in principle, be used to identify individuals at risk of suboptimal response due to cortical dopaminergic overactivation. Such biomarkers would complement existing clinical assessments and move the field closer to personalized pharmacotherapy, where dosing and adjunctive strategies are tailored not only to symptom severity but also to underlying network dynamics.
The new work also carries implications beyond Parkinson’s disease. Dopamine-modulating drugs are widely used across neurological and psychiatric conditions, often with highly variable outcomes. The methodological framework introduced here—linking individual neurophysiological response maps to neurochemical architectures—offers a generalizable approach for dissecting treatment heterogeneity in other disorders where neuromodulatory systems play a central role. Equally important is what the study cautions against. Increasing dopaminergic stimulation in the hope of achieving greater motor benefit may, in some patients, exacerbate off-target cortical effects that undermine overall efficacy. This insight argues for a more nuanced therapeutic philosophy, one that seeks an optimal balance rather than maximal dopaminergic drive. Finally, by separating rhythmic from aperiodic neural components, the authors demonstrate the value of refined analytical approaches in uncovering subtle but clinically meaningful effects. The findings highlight that treatment-related neurophysiological changes cannot be fully understood through coarse measures alone. Instead, careful dissection of oscillatory dynamics, interpreted within their neurochemical context, is essential for advancing both mechanistic understanding and clinical care.
Reference:
Alex I. Wiesman, Mikkel C. Vinding, Panagiota Tsitsi, Per Svenningsson, Josefine Waldthaler, Daniel Lundqvist. Cortical Effects of Dopamine Replacement Account for Clinical Response Variability in Parkinson’s Disease. Movement Disorders, 2025; DOI: 10.1002/mds.30200

