
Significance
A brief interruption of arterial inflow, followed by release, sets off a redistribution of blood across the skin microvasculature that depends strongly on depth. Superficially and deeper down, vessels do not behave in lockstep and some capillaries widen quickly, others respond later, and some barely respond at all. The timing matters because vessel size matters but in practice this entire sequence is usually compressed into a single number. During post-occlusive reactive hyperemia, that compression hides the way endothelial regulation actually breaks down or compensates at the scale where pathology often first appears. Microvascular endothelial dysfunction has been tied for years to cardiovascular risk, metabolic disorders, and smoking-related damage, with a growing body of work suggesting that it shows up before dysfunction of larger arteries becomes detectable. That idea is widely accepted. Still, most routine assessments continue to focus on macrovascular responses. The reason is not conceptual resistance so much as technical limitation. Non-invasive tools that can be deployed easily in humans do not resolve individual microvessels in vivo. Techniques based on laser Doppler flowmetry, near-infrared spectroscopy, or tissue spectrometry collect optical signals from tissue volumes that contain many thousands of capillaries, all oriented differently and carrying different flow histories. Once those signals are averaged, heterogeneity disappears. Depth-dependent effects disappear as well, even though endothelial signaling is not uniform across vessel classes. The skin should be an obvious window into human microvascular behavior. It is accessible, repeatable, and structurally organized. Even so, dynamic measurements remain difficult. Optical coherence tomography can image small vessels, but acquisition times are slow enough that only a few snapshots can be taken during a hyperemic response. What happens in between has to be inferred. Motion between scans introduces additional uncertainty, and axial projection artifacts complicate interpretation when depth really matters. The result is a partial view at best. Optoacoustic mesoscopy moves some of these constraints by combining optical absorption contrast with ultrasound detection, pushing spatial resolution into a range that scattering-limited optics cannot reach. Earlier implementations established sensitivity to microvascular structure in inflammatory and vascular disease. Functional measurements, though, remained limited by speed. Endothelial responses during hyperemia evolve on the order of seconds. Imaging that process demands acquisition rates that follow the biology without giving up spatial detail or usable penetration. Reaching that balance is the central technical challenge.
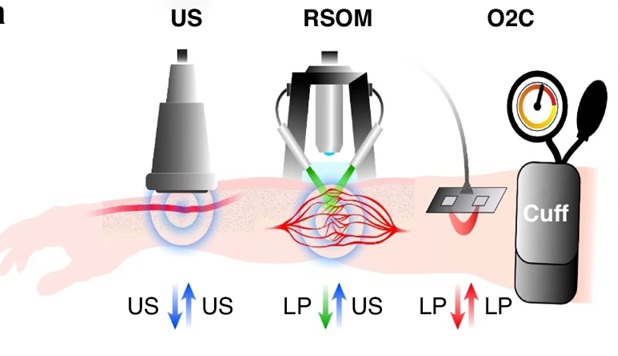
A recent research paper published in light: science & applications and conducted by Hailong He, Angelos Karlas, Nikolina-Alexia Fasoula, Chiara Fischer, Ulf Darsow, Michael Kallmayer, Juan Aguirre, Hans-Henning Eckstein & led by Professor Vasilis Ntziachristos from the Technical University of Munich in Germany, the researchers developed an accelerated optoacoustic mesoscopy framework capable of resolving individual skin capillaries during reactive hyperemia. The method combines coaxial illumination with adaptive scanning to balance volumetric context and high temporal resolution. They defined depth-specific dynamic parameters that quantify endothelial responses beyond bulk perfusion metrics. The system enables non-invasive, repeatable assessment of microvascular function at single-capillary resolution. The research team implemented an accelerated optoacoustic mesoscopy approach that combined coaxial illumination with adaptive scanning strategies to observe skin microvasculature during reactive hyperemia. By alternating between volumetric scans and rapid line scans, the investigators captured both three-dimensional vascular architecture and fast cross-sectional dynamics within the same anatomical region and this dual-mode strategy allowed spatial context to anchor temporal measurements.
Using the new system, the authors conducted forearm occlusion tests in healthy volunteers, smokers, and individuals with diagnosed cardiovascular disease. The researchers observed that arterial occlusion progressively reduced optoacoustic signal from dermal vessels while epidermal melanin remained stable, providing an internal reference. Upon cuff release, vascular signals rebounded sharply, accompanied by the appearance of vessels not visible at baseline. Individual capillaries expanded by different amounts and on different schedules, with larger vessels showing stronger dilation and smaller vessels displaying delayed recovery. The investigators quantified these behaviors by extracting intensity-based measures from depth-segmented data. Instead of collapsing signals across the dermis, they evaluated subpapillary and reticular layers separately. This choice exposed systematic differences: superficial capillaries reacted earlier to occlusion yet recovered more slowly after reperfusion, while deeper vessels reached peak response sooner once flow resumed. That staggered timing persisted across subjects, which indicate that it reflected physiological organization.
The team introduced three parameters derived from continuous optoacoustic traces: maximum volume change, hyperemia ratio, and time-to-peak. The authors applied these metrics to compare risk groups. In smokers, all three measures shifted relative to non-smokers, with the largest deviations occurring in the subpapillary dermis. Volunteers with cardiovascular disease exhibited further reductions, again concentrated in superficial layers. At the same time, structural metrics such as total dermal blood volume showed little separation between groups. The researchers directly compared these findings with simultaneous laser Doppler and spectrometric measurements. Those conventional signals tracked gross perfusion changes but failed to discriminate between smokers and non-smokers at the microvascular level. The contrast exposed a limitation that the study did not resolve but clearly acknowledged: bulk flow metrics respond quickly, yet they obscure the slower reconstitution of capillary networks that optoacoustic measurements detect. The trade-off favors sensitivity to function over simplicity of readout, a choice that shapes how endothelial health can be interpreted. Repeat measurements across days showed tighter clustering for optoacoustic-derived parameters than for optical flow measurements, reinforcing that resolving vessels individually reduces variability introduced by orientation and scattering. The experiments collectively demonstrated that endothelial dysfunction expresses itself through altered capillary dynamics long before gross morphology changes, and that these alterations vary systematically with skin depth and disease state.
To summarize, the new findings of Professor Vasilis Ntziachristos and colleagues matter because they reframe endothelial dysfunction as a spatially and temporally structured process and shows that superficial and deeper dermal capillaries respond differently to the same vascular challenge which challenges the assumption that microvascular beds behave as homogeneous compartments. For cardiovascular research, the ability to detect dysfunction at the level of single capillaries offers a path toward earlier stratification of risk. Smoking and established cardiovascular disease altered dynamic parameters without producing obvious structural differences, implying that function degrades before architecture follows. This ordering aligns with clinical observations but had not been demonstrated directly in humans at this scale. The implication is conditional but important: functional markers derived from capillary dynamics may identify vulnerability during a window when intervention remains feasible.
The depth-resolved nature of the measurements also carries design consequences for future studies. Many interventions target endothelial signaling pathways that may not affect all vessels equally. A method that separates responses by layer and vessel size allows investigators to ask whether therapies normalize timing, amplitude, or coordination of capillary recruitment and this distinction could influence how treatment efficacy is defined and monitored.
From a technological standpoint, we believe the study illustrates how accelerating acquisition changes what questions become askable. High temporal resolution did not simply refine existing metrics; it exposed delays and recovery patterns that averaged methods cannot infer. At the same time, the approach accepts limits. Line scanning samples a thin region to achieve speed, leaving lateral heterogeneity partially unobserved. Scaling to larger fields while preserving temporal fidelity remains an open engineering constraint and clinical translation depends on whether such measurements remain robust across broader populations and longitudinal settings. The system operates without contrast agents and within established safety limits, which lowers barriers to repeated use. Still, the work frames its claims conservatively, treating biomarkers as candidates whose relevance must be tested against outcomes not replace existing diagnostics.

Reference
He H, Karlas A, Fasoula NA, Fischer C, Darsow U, Kallmayer M, Aguirre J, Eckstein HH, Ntziachristos V. Single-capillary endothelial dysfunction resolved by optoacoustic mesoscopy. Light Sci Appl. 2026 Jan 3;15(1):37. doi: 10.1038/s41377-025-02103-6.